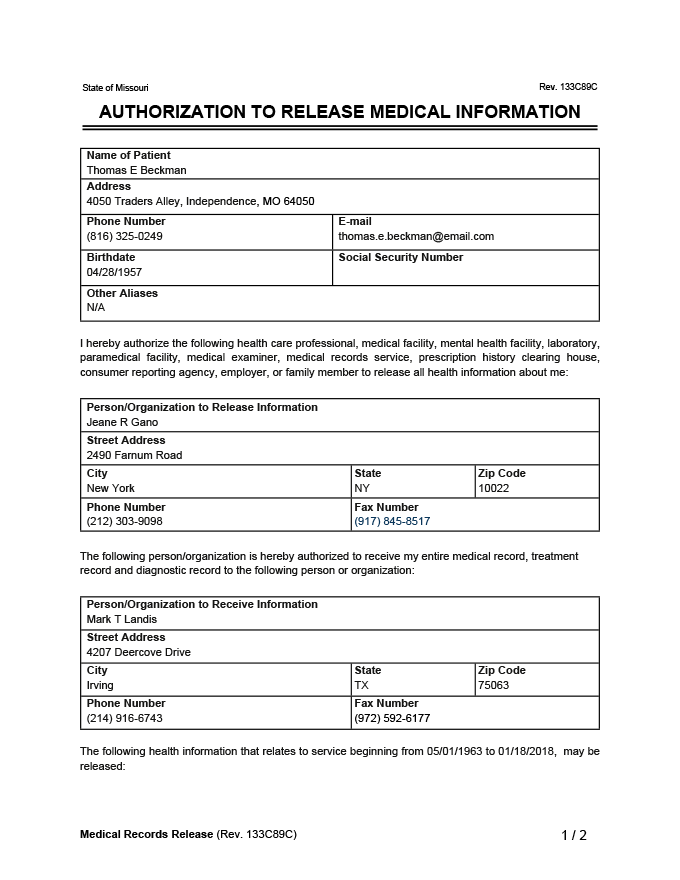
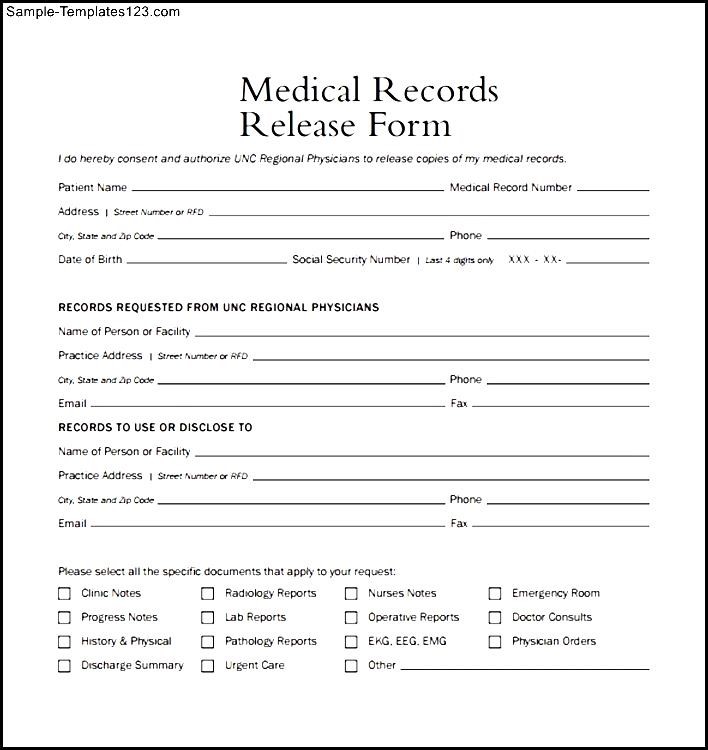
Generic Printable Medical Records Release Authorization Form - Web use our medical records release authorization form to allow the release of your medical information to yourself or anyone else who may need it. Web authorization to disclose personal health information release form. If any sections are left blank, this form will be invalid and it will not be possible for your health. Web a hipaa release form, also known as a hipaa authorization or hipaa consent form, is a legal document signed by an individual to grant permission for their. Web this authorization is given in compliance with the federal consent requirements for release of alcohol or substance abuse records of 42 cfr 2.31, the restrictions of which have. Web i hereby authorize the following health care professional, medical facility, mental health facility, laboratory, paramedical facility, medical examiner, medical records service,. Web the medical records release authorization is the disclosure of the members of the family or next of kin to whom a person would wish to have access to his medical. Web general medical records release and authorization for use or disclosure of protected health information ms 1 04 ms 100400. The form must allow them to request their personal health information (phi) or grant a third party permission to release it. Web direct access to pdf of hipaa release.
Generic Medical Records Release Form download free documents for PDF
Web authorization to use and/or disclose protected health information. The information used or disclosed pursuant to this authorization may be subject to. Web mail or.

Free Medical Release Form Template Continuum
Web the form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Please complete.
Free Medical Records Release (HIPAA) Form PDF & Word
Web the form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Web a.

Authorization to Release Medical Records Fill and Sign Printable
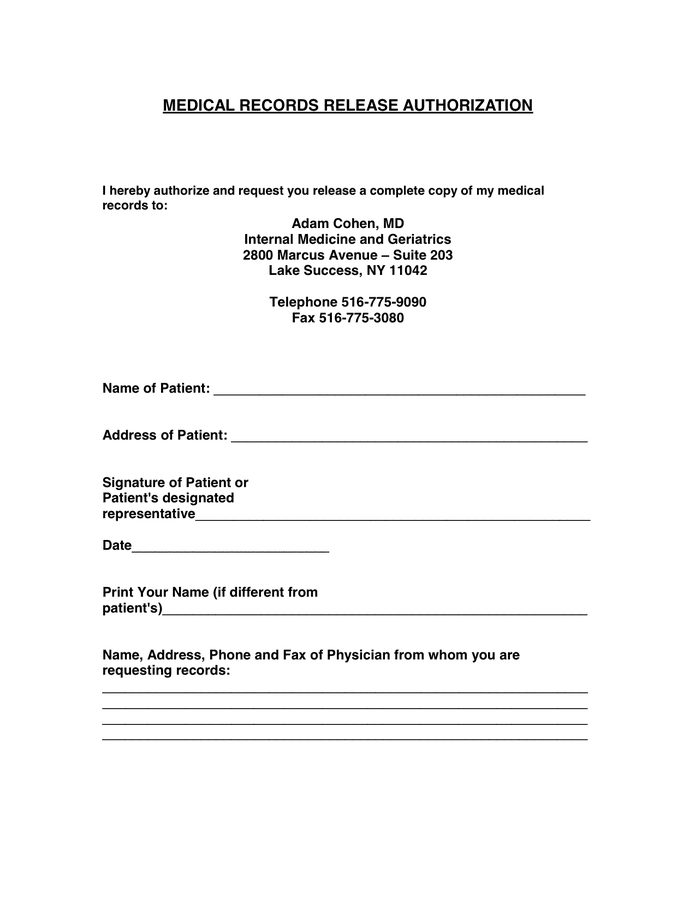
Free immediate download of pdf. To request release of medical information please complete and sign this form. Web medical records release forms are formal documents.
Generic Medical Records Release Form download free documents for PDF
Web jotform’s medical records release authorization template allows you to quickly and easily gather signatures from patients or parents or guardians in order to release..
Free Medical Records Release Authorization Form (Waiver) HIPAA PDF
Web the form authorizes release of information in accordance with the health insurance portability and accountability act, 45 cfr parts 160 and 164; Web i.
Free Medical Records Release (HIPAA) Form PDF & Word
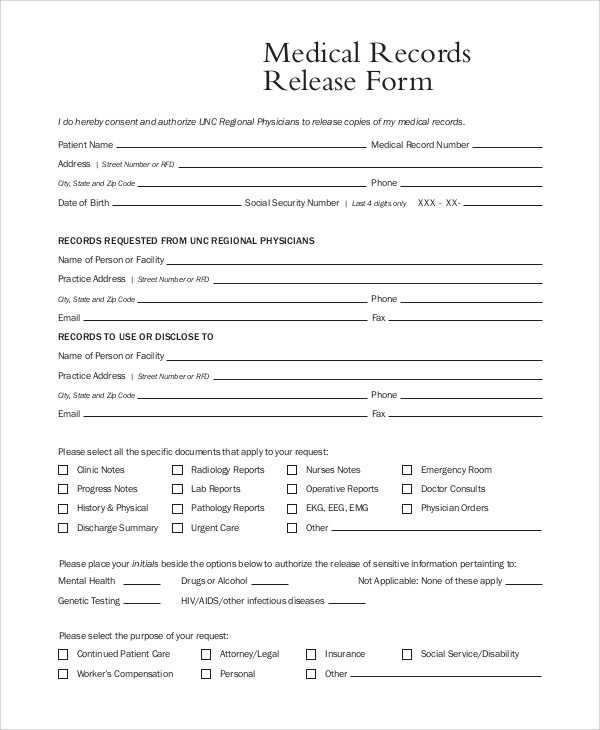
Web this authorization is given in compliance with the federal consent requirements for release of alcohol or substance abuse records of 42 cfr 2.31, the.
MEDICAL RECORDS RELEASE AUTHORIZATION in Word and Pdf formats
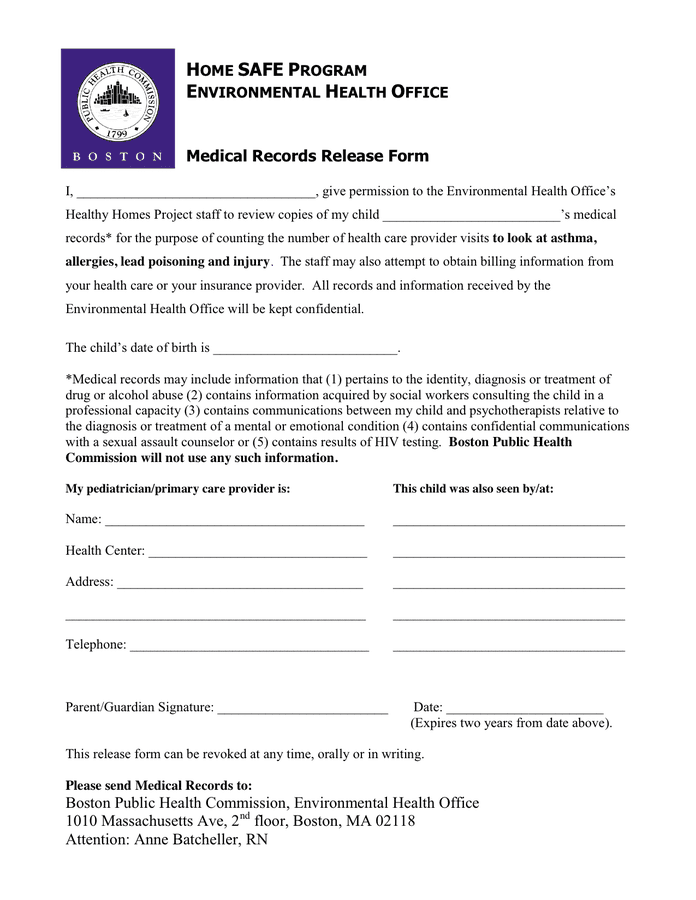
Web the medical records release authorization is the disclosure of the members of the family or next of kin to whom a person would wish.
Generic Medical Records Release Form Template Business
Web the medical records release authorization is the disclosure of the members of the family or next of kin to whom a person would wish.
FREE 9+ Sample Medical Records Release Forms in PDF MS Word
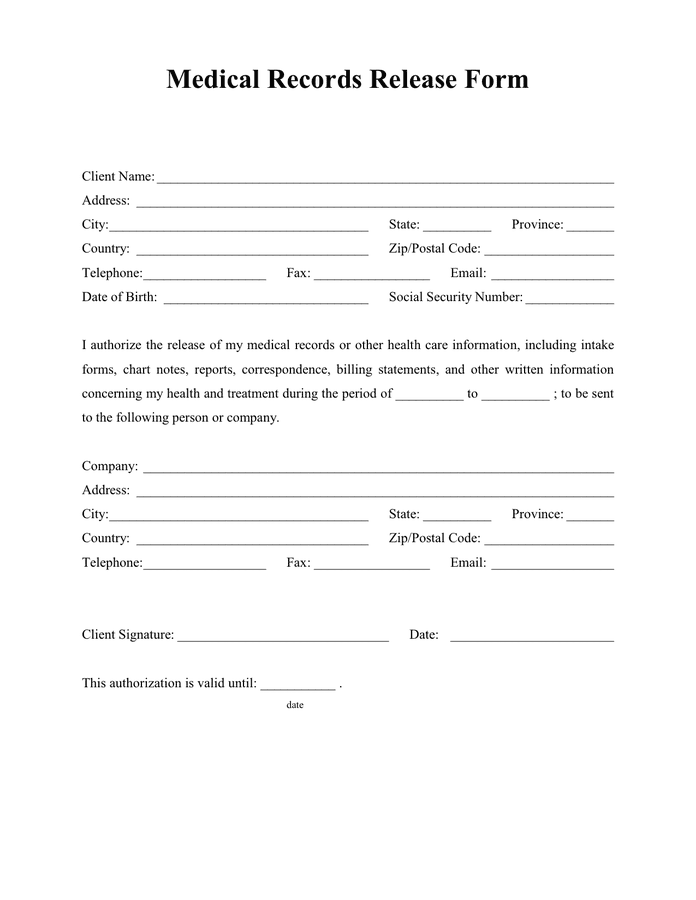
Web use our medical records release authorization form to allow the release of your medical information to yourself or anyone else who may need it..
Web The Form Authorizes Release Of Information In Accordance With The Health Insurance Portability And Accountability Act, 45 Cfr Parts 160 And 164;
Web the medical records release authorization is the disclosure of the members of the family or next of kin to whom a person would wish to have access to his medical. Web a medical records release form is a formal document that legitimizes the sharing of a patient's medical information between healthcare providers, insurance. Web jotform’s medical records release authorization template allows you to quickly and easily gather signatures from patients or parents or guardians in order to release. If any sections are left blank, this form will be invalid and it will not be possible for your health.
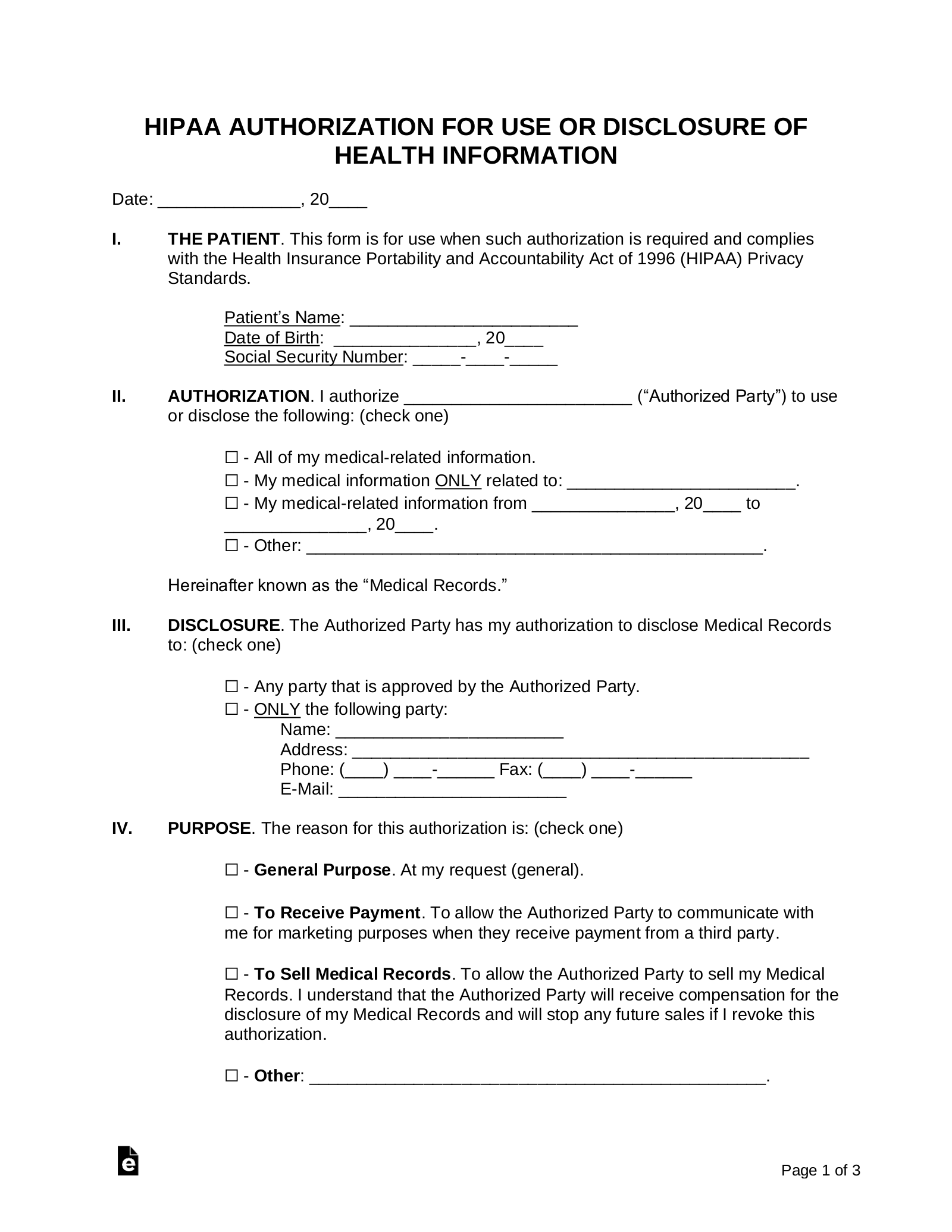
I Authorize ________________________ (“Authorized Party”) To Use Or Disclose The Following:
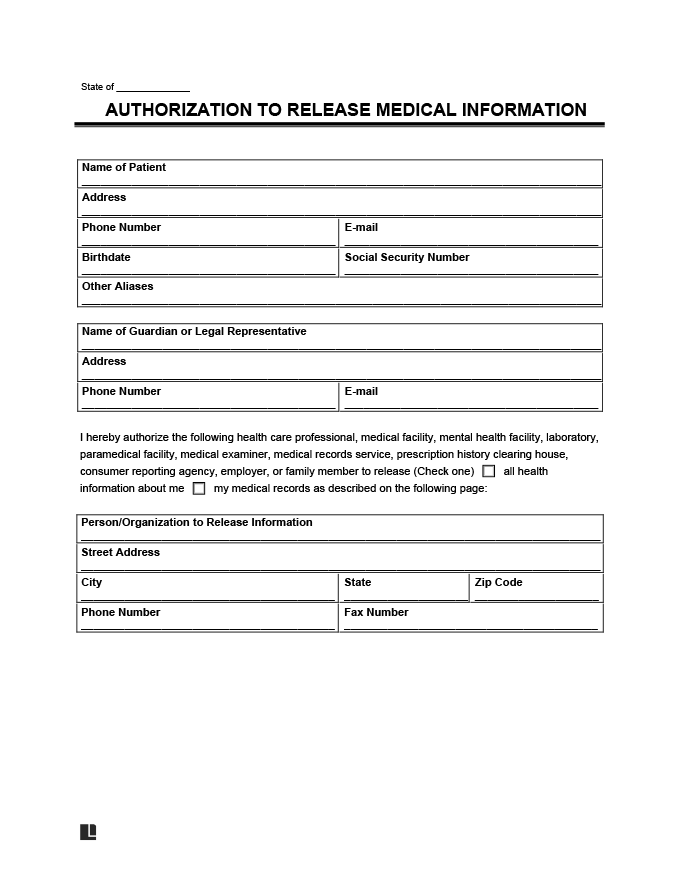
Web mail or fax release form to: Web a hipaa authorization form to release medical records must be obtained from a patient or their personal representative before any protected health information. Web i hereby authorize the following health care professional, medical facility, mental health facility, laboratory, paramedical facility, medical examiner, medical records service,. Web authorization to disclose personal health information release form.
The Information Used Or Disclosed Pursuant To This Authorization May Be Subject To.
A hipaa release form must be obtained from a patient before their protected health information. Web a hipaa release form, also known as a hipaa authorization or hipaa consent form, is a legal document signed by an individual to grant permission for their. Web use our medical records release authorization form to allow the release of your medical information to yourself or anyone else who may need it. To request release of medical information please complete and sign this form.
Web Authorization For Release Of Medical Records.
Web authorization to use and/or disclose protected health information. To fill out a hipaa release form, a patient must choose the appropriate document. Web direct access to pdf of hipaa release. Web this authorization is given in compliance with the federal consent requirements for release of alcohol or substance abuse records of 42 cfr 2.31, the restrictions of which have.