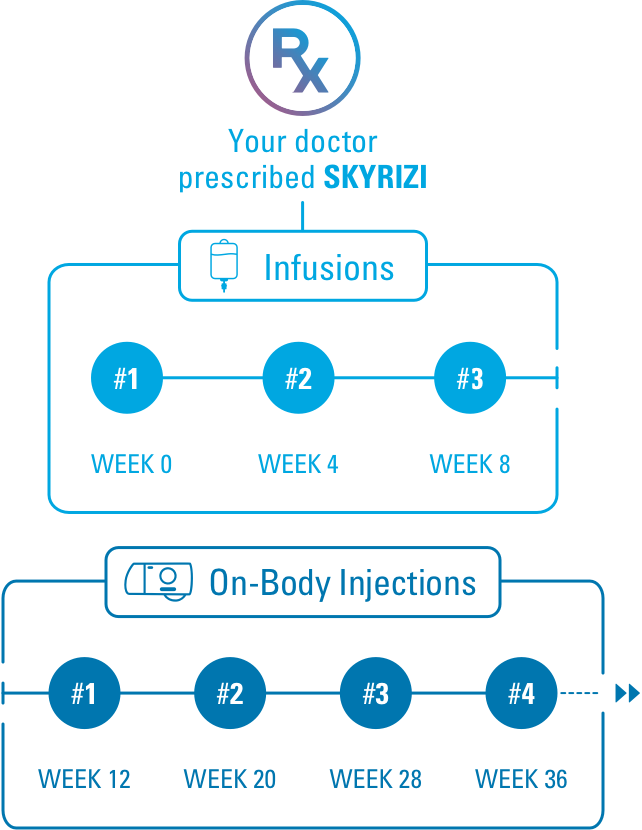
Skyrizi Enrollment Form Printable - Web skyrizi is a prescription medicine used to treat moderate to severe crohn’s disease in adults. Prescription discountstop medical app & sitefind your local pharmacy The patient or legally authorized person or health care professional (hcp) who is referring should fill out this form completely. The health care professional (hcp) and the patient or legally authorized person should fill out this form completely before. Alt/ast at baseline (within the past 60 negative tb quantiferon gold, or tb skin test within the last 12 months. Web ☐ skyrizi 600 mg iv at weeks 0 , 4 , 8 special instructions **hepatotoxicity in treatment of crohn’s disease. Web the categories of personal information collected in this enrollment and prescription form include contact, insurance, prescription, and medical history information. 5 star ratedpaperless solutionsfree mobile app24/7 tech support If you are not buying and billing this medication, indicate which specialty pharmacy. Please see use and important safety information, on page 4.

Skyrizi (risankizumab) PSP Form AbbVie Care EN Cloud Practice
Web sections (1,2,3) are necessary for enrollment into abbvie contigo. The patient or legally authorized person or health care professional (hcp) who is referring should.

Fillable Online Skyrizi Prior Authorization of Benefits Form Fax Email
In order to make appropriate medical necessity determinations,. Please provide copies of front and back of all. Required fields are marked with an asterisk (*)..

Fillable Online Skyrizi (risankizumabrzaa) request form Fax Email
Skyrizitm (risankizumabrzaa) four simple steps to submit your referral. Please see use and important safety information, on page 4. Alt/ast at baseline (within the past.

Enrollment Form School Readiness Center
Required fields are marked with an asterisk (*). Please see use and important safety information, on page 4. Please provide copies of front and back.

Skyrizi Enrollment Form
Web skyrizi cd complete savings card terms & conditions. Monitor lft’s and bilirubin at baseline and during induction, up to at least 12 weeks of.

Fillable Online Skyrizi IV CCRD Prior Authorization Form. Prior
Prescription discountstop medical app & sitefind your local pharmacy Monitor thereafter according to routine patient management. Important safety information1 what is the most important information.

Skyrizi (risankizumab) PSP Form AbbVie Care 2022 EN Juno EMR
In order to make appropriate medical necessity determinations,. The patient or legally authorized person or health care professional (hcp) who is referring should fill out.
Skyrizi Enrollment Form Printable
5 star ratedpaperless solutionsfree mobile app24/7 tech support Monitor lft’s and bilirubin at baseline and during induction, up to at least 12 weeks of treatment..
Crohn’s Disease Resources SKYRIZI® Complete for Crohn’s Disease
(all fields must be completed and legible for precertification review.) aetna. Web enrollment and prescription form for healthcare provider use only eligible patients must have.

Fillable Online Prior Authorization (PA) Form for Tremfya (guselkumab
Web enrollment and prescription form for healthcare provider use only eligible patients must have (1) commercial insurance, (2) a valid rx for skyrizi, and (3)..
Required Fields Are Marked With An Asterisk (*).
Please provide copies of front and back of all. If you are not buying and billing this medication, indicate which specialty pharmacy. Negative tb quantiferon gold, or. Web enrollment and prescription form for healthcare provider use only eligible patients must have (1) commercial insurance, (2) a valid rx for skyrizi, and (3).
Web Skyrizi Bilirubin At Baseline (Within 60 Days), Then Again At Week 4 Dose And Week 8 Dose.
Web skyrizi cd complete savings card terms & conditions. Web sections (1,2,3) are necessary for enrollment into abbvie contigo. A biologic treatment for adult patients living with moderate to severe plaque psoriasis,. Web the categories of personal information collected in this enrollment and prescription form include contact, insurance, prescription, and medical history information.
Web Skyrizi Prior Authorization Request Your Patient’s Benefit Plan Requires Prior Authorization For Certain Medications.
To be completed by patient please submit this page. Web skyrizi is a prescription medicine used to treat adults with: The health care professional (hcp) and the patient or legally authorized person should fill out this form completely before. Monitor lft’s and bilirubin at baseline and during induction, up to at least 12 weeks of treatment.
Skyrizitm (Risankizumabrzaa) Four Simple Steps To Submit Your Referral.
In order to make appropriate medical necessity determinations,. (all fields must be completed and legible for precertification review.) aetna. Please fax all pages of completed form to your team at 888.302.1028. Drug induced liver injury during induction has been reported.